Summary
Background
There is major concern about the impact of the global COVID-19 outbreak on mental health. Several studies suggest that mental health deteriorated in many countries before and during enforced isolation (ie, lockdown), but it remains unknown how mental health has changed week by week over the course of the COVID-19 pandemic. This study aimed to explore the trajectories of anxiety and depression over the 20 weeks after lockdown was announced in England, and compare the growth trajectories by individual characteristics.
Methods
In this prospective longitudinal observational study, we analysed data from the UCL COVID-19 Social Study, a panel study weighted to population proportions, which collects information on anxiety (using the Generalised Anxiety Disorder assessment) and depressive symptoms (using the Patient Health Questionnaire) weekly in the UK since March 21, 2020. We included data from adults living in England who had at least three repeated measures between March 23 and Aug 9, 2020. Analyses were done using latent growth models, which were fitted to account for sociodemographic and health covariates.
Findings
Between March 23, and Aug 9, data from over 70 000 adults were collected in the UCL COVID-19 Social Study. When including participants living in England with three follow-up measures and no missing values, our analytic sample consisted of 36 520 participants. The average depression score was 6·6 (SD=6·0, range 0–27) and the average anxiety score 5·7 (SD=5·6, range 0–21) in week 1. Anxiety and depression levels both declined across the first 20 weeks following the introduction of lockdown in England (b=–1·93, SE=0·26, p<0·0001 for anxiety; b=–2·52, SE=0·28, p<0·0001 for depressive symptoms). The fastest decreases were seen across the strict lockdown period (between weeks 2 and 5), with symptoms plateauing as further lockdown easing measures were introduced (between weeks 16 and 20). Being a woman or younger, having lower educational attainment, lower income, or pre-existing mental health conditions, and living alone or with children were all risk factors for higher levels of anxiety and depression at the start of lockdown. Many of these inequalities in experiences were reduced as lockdown continued, but differences were still evident 20 weeks after the start of lockdown.
Interpretation
These data suggest that the highest levels of depression and anxiety occurred in the early stages of lockdown but declined fairly rapidly, possibly because individuals adapted to circumstances. Our findings emphasise the importance of supporting individuals in the lead-up to future lockdowns to try to reduce distress, and highlight that groups already at risk for poor mental health before the pandemic have remained at risk throughout lockdown and its aftermath.
Funding
Nuffield Foundation, UK Research and Innovation, Wellcome Trust.
Introduction
and a call for urgent mental health research.
Stay-at-home and quarantine orders issued by governments led to the largest enforced isolation period in human history. Infections and deaths from the virus led to psychological stress and bereavement. Furthermore, many individuals globally faced high levels of adversities, from challenges meeting basic needs (eg, accessing food, water, and safe accommodation) to financial problems (including job losses, income cuts, and inability to pay bills).
,
These findings echo those from studies of previous epidemics such as the epidemic of severe acute respiratory syndrome (SARS), during which individuals who had to quarantine experienced increases in symptoms of depression and post-traumatic stress disorder.
,
,
,
However, what remains unclear is the trajectory of mental health across the course of the COVID-19 pandemic. The studies on SARS suggested that mental health worsened during periods of quarantine or enforced isolation.
,
However, some sources suggest that during the COVID-19 pandemic, mental health deteriorated before the stay-at-home orders (ie, lockdowns) were introduced.
,
,
Given these findings, what remains to be understood is whether mental health continued to worsen as lockdown continued, or whether there were any patterns of stabilisation or improvement. Similarly, it is unknown whether mental health improved or whether new stressors arose for individuals as lockdown measures were eased. These are important questions as understanding the patterns of mental health across lockdowns could help mental health services and voluntary organisations to plan for future waves of the virus. Furthermore, understanding how humans respond to periods of enforced isolation could enhance our understanding of the effect of social isolation on mental health.
Evidence before this study
We searched PubMed for articles published in English between Jan 1, 2020, and Sept 14, 2020, using the following keywords: “COVID*” OR “coronavirus” and “anxiety” OR “depression” OR “mental health” OR “mental illness” OR “distress”. Studies using data from representative cohort studies revealed the substantial impact of the COVID-19 pandemic on levels of depression, anxiety, and mental distress, showing increases in average scores of symptoms of psychological distress from before the pandemic to during the pandemic, and a rise in the proportion of people experiencing clinically significant levels of mental illness. But there was a gap in the evidence in understanding how mental health changed week by week over the course of the COVID-19 pandemic.
Added value of this study
This study shows that mental health was adversely affected in the 20 weeks following the start of the first lockdown in England. However, since the commencement of the first lockdown, many people began to experience improvements in mental health. Many known risk factors for poorer mental health were apparent early in lockdown, such as women, younger adults, and individuals with lower educational attainment. As mental health improved, the difference between these vulnerable groups and people without these risk factors reduced but was still evident 20 weeks after the start of lockdown.
Implications of all the available evidence
Our findings, together with previous studies comparing populations before and after the start of the COVID-19 pandemic, emphasise the importance of supporting individuals to try to reduce distress early in a pandemic. Many inequalities in mental health experiences persisted and emotionally vulnerable groups have remained at risk throughout lockdown and its aftermath. These groups could benefit from more targeted mental health support as the pandemic continues.
,
Findings from previous epidemics have suggested that many of these factors have also been risk factors for worse mental health during periods of isolation,
and data about the COVID-19 pandemic have echoed these findings.
,
,
,
,
,
Similarly, there has been some indication that pre-existing psychiatric conditions are a risk factor for poorer mental health outcomes,
which has also been echoed by data from the COVID-19 pandemic.
,
However, previous research has focused on cross-sectional data or discrete timepoints during the pandemic. The effect of these risk factors on the trajectories of mental health during the COVID-19 pandemic remains unknown. Identifying such risk factors is important to ascertain who is most in need of support both during the ongoing pandemic and in preparing for future pandemics.
Therefore, this study had two main aims: first, to explore trajectories of anxiety and depressive symptoms over the strict lockdown period and as lockdown was eased; and second, to identify who was most at risk of poorer trajectories of mental health across this period.
Methods
Study design and participants
The research questions in the COVID-19 Social Study built on patient and public involvement as part of the UKRI MARCH Mental Health Research Network, which highlighted priority research questions and measures for this study. Patients and the public were additionally involved in the recruitment of participants and the dissemination of findings.
Procedures
with 4-point responses ranging from “not at all” to “nearly every day”. Scores of 0–4 are thought to represent minimal anxiety, 5–9 mild anxiety, 10–14 moderate anxiety, and 15–21 severe anxiety.
Depressive symptoms were measured using the Patient Health Questionnaire (PHQ-9), a standard 9-item instrument for diagnosing depression in primary care,
with 4-point responses ranging from “not at all” to “nearly every day”. Scores of 0–4 suggest minimal depression, 5–9 mild depression, 10–14 moderate depression, 15–19 moderately severe depression, and 20–27 severe depression.
The validated measures of both the GAD-7 and PHQ-9 ask respondents to focus on the past 2 weeks, but because the COVID-19 Social Study involved weekly reassessments, we asked participants to focus just on the past week.
We included sociodemographic variables as time-invariant covariates, namely, gender (men vs women), age groups (18–29 years, 30–45 years, 46–59 years, and 60 years or older), ethnicity (white vs BAME), education (General Certificate of Secondary Education or lower education [equivalent to education to the age of 16 years], A levels or equivalent [equivalent to education to the age of 18 years], undergraduate degree or above [further education after the age of 18 years]), income (household income <£30 000 vs ≥£30 000), and living arrangement (alone, living with others but no children in the household, living with others including children in the household). We assessed diagnosed mental illness (as another time-invariant covariate) by asking participants “Do you have any of the following medical conditions”, with the responses being “clinically-diagnosed depression”, “clinically-diagnosed anxiety”, and “another clinically-diagnosed mental health problem”. Participants could select as many categories as applied and the responses were binarised into “diagnosed mental illness” or “no diagnosed mental illness”. Participants were also asked whether they had had COVID-19 (“yes, diagnosed and recovered/still ill”, “not formally diagnosed but suspected”, or “not that I know of/no”). However, only a very small percentage of the sample (0·02–0·88% each week) reported being formally diagnosed with a test due to limitations on testing in the early months of the pandemic; therefore, we did not include experience of COVID-19 in the analyses. Further detail on the measures is available in the study user guide.
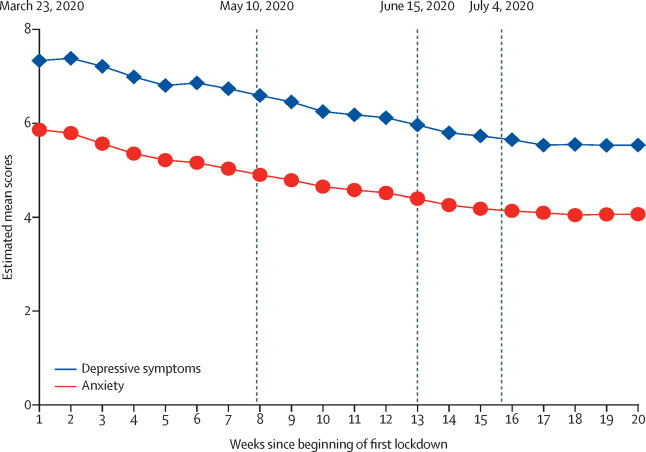
Figure 1Predicted growth trajectories of estimated mean anxiety and depressive symptom scores
Scores on anxiety were measured using the Generalised Anxiety Disorder assessment (range of scores: 0–21) and scores on depressive symptoms were measured using the Patient Health Questionnaire (range of scores: 0–27). On March 23, the first lockdown commenced in England. On May 10, it was announced that strict lowdown was being eased. On June 15, non-essential retail was reopened. On July 4, further public amenities were reopened.
Statistical analysis
1-1
1-2
1-3
The correlation between outcome measures is shown in the appendix (p 4). Unweighted and weighted descriptive statistics by week are shown in the appendix (p 4). Descriptive analyses were done using Stata version 15. The latent growth models were fitted in Mplus version 8.
Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. All researchers listed as authors are independent from the funders and all final decisions about the research were taken by the investigators and were unrestricted.
Results
Table 1Descriptive statistics of the explanatory variables for the 36 520 participants at their baseline assessment
Table 2Levels of anxiety and depressive symptoms in the sample in week 1 (weighted)
Data are mean (SD) or n (%). Not all participants started the study in week 1, so this table does not represent the full number of participants included in the statistical sample. Scores on depressive symptoms were measured using the Patient Health Questionnaire (range of scores: 0–27). Scores of 0–4 suggest minimal depression, 5–9 mild depression, 10–14 moderate depression, 15–19 moderately severe depression, and 20–27 severe depression. Scores on anxiety were measured using the Generalised Anxiety Disorder assessment (range of scores: 0–21). Scores of 0–4 suggest minimal anxiety, 5–9 mild anxiety, 10–14 moderate anxiety, and 15–21 severe anxiety.
Table 3Estimated effects of the covariates on the intercepts and slopes from the conditional multiprocess latent growth model
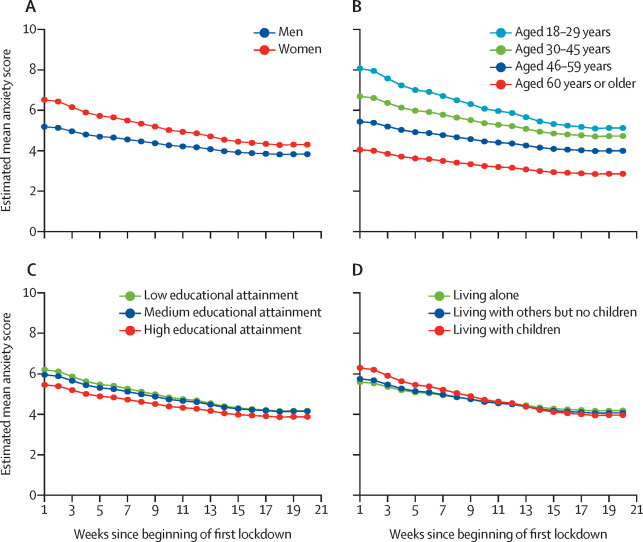
Figure 2Predicted growth trajectories of mean anxiety scores by individual characteristics
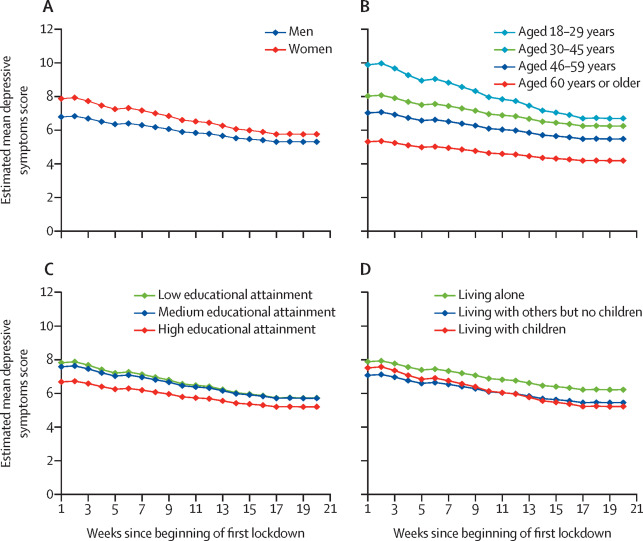
Figure 3Predicted growth trajectories of mean depressive symptom scores by individual characteristics
Discussion
This study explored trajectories of anxiety and depression across the first 20 weeks following the start of the first lockdown response to the COVID-19 pandemic in England. Results show that anxiety and depressive symptoms both declined across the first 20 weeks following the introduction of lockdown in England. The fastest decreases were seen across the strict lockdown period, with symptoms plateauing as further lockdown easing measures were introduced. Being female or younger, having lower educational attainment, lower income, or pre-existing mental health conditions, and living alone or with children were all risk factors for higher levels of anxiety and depressive symptoms at the start of lockdown. Many of these inequalities in experiences were reduced as lockdown continued, but differences were still evident 20 weeks after the start of lockdown.
,
The fact that levels of mental health did not continue to worsen in this period is slightly at odds with data from previous epidemics, in which mental health was found to worsen during (or as a result of) quarantine.
However, there are several key differences between this pandemic and previous epidemics. First, for the majority of people in England during lockdown, some trips outside of the home were permissible, whereas previous studies looked at quarantines in which movement was more restricted, albeit typically for much smaller numbers of people. The more restricted quarantines of previous epidemics might have led to a harsher psychological experience. Second, there was substantial previous warning in England that a lockdown was likely to happen given patterns in other European countries. Individuals appeared to have become psychologically affected before the lockdown announcement (and many individuals self-isolated voluntarily before lockdown officially started). This anticipation means that much of the psychological toll was already being experienced before individuals were forced to isolate.
Finally, the proliferation of online and home-based leisure activities and the extensive use of virtual and digital communication during the COVID-19 pandemic might have helped to ease the burden of lockdown itself, in contrast to previous epidemics in which the fear of missing out was reported to be a challenge.
Indeed, fear of missing out (which is associated with depression, distraction, and somatic symptoms
) might also have been reduced because of the global nature of this pandemic, compared with the restricted nature of quarantines in previous pandemics. The improvements in mental health over this strict lockdown period suggest a process of adaptation that bears similarities to literature on other types of isolation: for example, some studies of incarceration have shown that depression levels can stabilise and even decrease month after month as new coping strategies emerge.
It is further possible that measures to safeguard jobs and finances taken in the UK might have helped to reduce specific anxieties. The lockdown itself might also have reduced worries about individuals or their friends or families catching the virus, especially after the first 2 weeks of lockdown when individuals could be more confident that they were outside of the incubation period.
,
,
but our data show that these groups have also had faster improvements in their symptoms. This finding could indicate a more challenging psychological experience early on in lockdown (eg, as many women balanced child care and working from home) or a higher initial reactivity to events among these groups. By contrast, adults living alone had consistently worse levels of depressive symptoms, which could be related to higher levels of loneliness due to social restrictions.
However, individuals living with children had higher levels of anxiety and depressive symptoms initially than individuals living with other adults, but a faster rate of improvement, potentially due to the growing public awareness of research suggesting that children were less affected by COVID-19.
Similarly, individuals with lower household income had consistently worse mental health than individuals with a higher household income, which has been proposed to be linked to higher experiences of adversities such as job losses, decreases in household income, and challenges to pay bills.
But differences in mental health at baseline are probably attributable to pre-existing social inequalities that have been exacerbated over the past decade.
Although we found that individuals with mental illness had higher levels of depressive symptoms and anxiety at the start of lockdown (which is echoed in COVID-19 studies
,
,
from various countries), they had the same trajectories over the subsequent weeks. This finding suggests that mental illness did not necessarily predispose individuals to greater levels of emotional reactivity. It is possible that previous experience of mental illness or social isolation caused by previous mental illness meant individuals had experience of some of the requirements of lockdown or of applying coping strategies in stressful situations. But lockdown might also have enabled unhealthy coping strategies, so these hypotheses remain to be explored. Furthermore, future studies are recommended to look at specific types of psychiatric diagnoses in relation to mental health to identify whether particular psychopathologies are associated with poorer trajectories over the course of the pandemic. Our models suggested that ethnicity was not a risk factor for worse mental health. But the models adjusted simultaneously for multiple demographic factors including socioeconomic position, and socioeconomic position was related to poorer psychological experiences. Individuals from ethnic minority groups are disproportionately more likely to be from lower socioeconomic groups,
so they might still have been disproportionately affected. We used some binary categories in our analyses for ethnicity (and for other variables such as gender), but we recognise that such labels do not fully capture the experiences of different groups. Ethnic minority groups were under-represented in our data (although we did weight to increase the proportion of their responses). As a result, we did not have sufficient statistical power to look at the experiences of specific ethnic groups and our analysis did not explore the experiences of individuals with non-binary gender identities, but we recognise the need for and encourage and support future research on these areas.
Future studies could also consider how geographical factors including location within the UK, level of urbanisation, and area deprivation might have moderated psychological experiences during lockdown and whether experience of COVID-19 could have affected psychological response.
Overall, these findings suggest that the highest levels of depression and anxiety in England were in the early stages of lockdown but declined fairly rapidly following the introduction of lockdown, with improvements continuing as lockdown easing measures were introduced and then plateauing after the first 4 months. Many known risk factors for poorer mental health were associated with inequalities in mental health at the start of lockdown. However, some groups, including women, younger adults, and individuals with lower educational attainment, had faster improvements in symptoms, thereby reducing the differences between these vulnerable groups and other groups over time. Nevertheless, many inequalities in mental health experiences (such as inequalities by age and gender) did remain and emotionally vulnerable groups (such as individuals with existing mental health conditions or individuals living alone) have remained at risk throughout lockdown and its aftermath. As countries face potential future lockdowns, these data emphasise the importance of supporting individuals in the lead-up to lockdown to try to reduce distress; yet these data also suggest that individuals might be able to adapt relatively fast to the new psychological demands of life in lockdown. But because inequalities in mental health have persisted, it is key to find ways of supporting vulnerable groups during this pandemic.
DF, AS, and FB conceived and designed the study. FB analysed the data and DF wrote the first draft. All authors provided critical revisions. All authors read and approved the submitted manuscript. DF and FB accessed and verified the data.
We declare no competing interests.