
Raquel S. Mateus, PharmD Candidate
Depression can take several forms. To receive a diagnosis of depression, patients must have symptoms (TABLE 11) most of the day for at least 2 weeks.2 By discussing symptoms, treatment options, and adverse effects, pharmacists can help patients adhere to their treatment regimen.
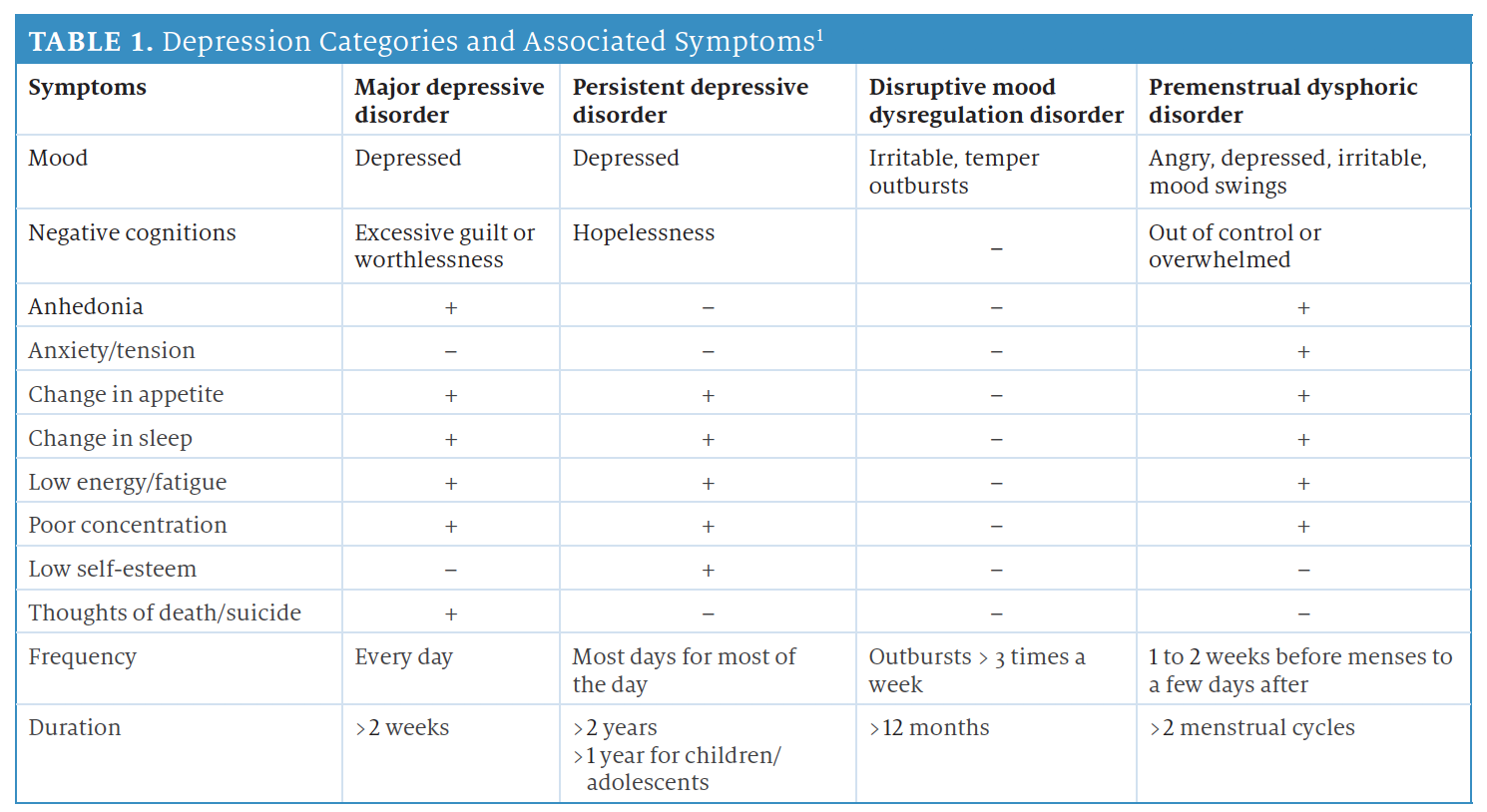
Some forms of depression develop under unique circumstances. For example, women may experience major depression during pregnancy or after delivery (postpartum depression). Seasonal affective disorder usually occurs in fall and winter and typically goes away during the spring and summer. Psychotic depression occurs when a person has severe depression plus some form of psychosis, such as delusions or hallucinations.2
TREATMENT OPTIONS
Initial treatment includes medications (TABLE 23-5), psychotherapy, or both. Brain stimulation therapy is usually reserved for patients who do not respond to multiple treatments (treatment-resistant depression).2
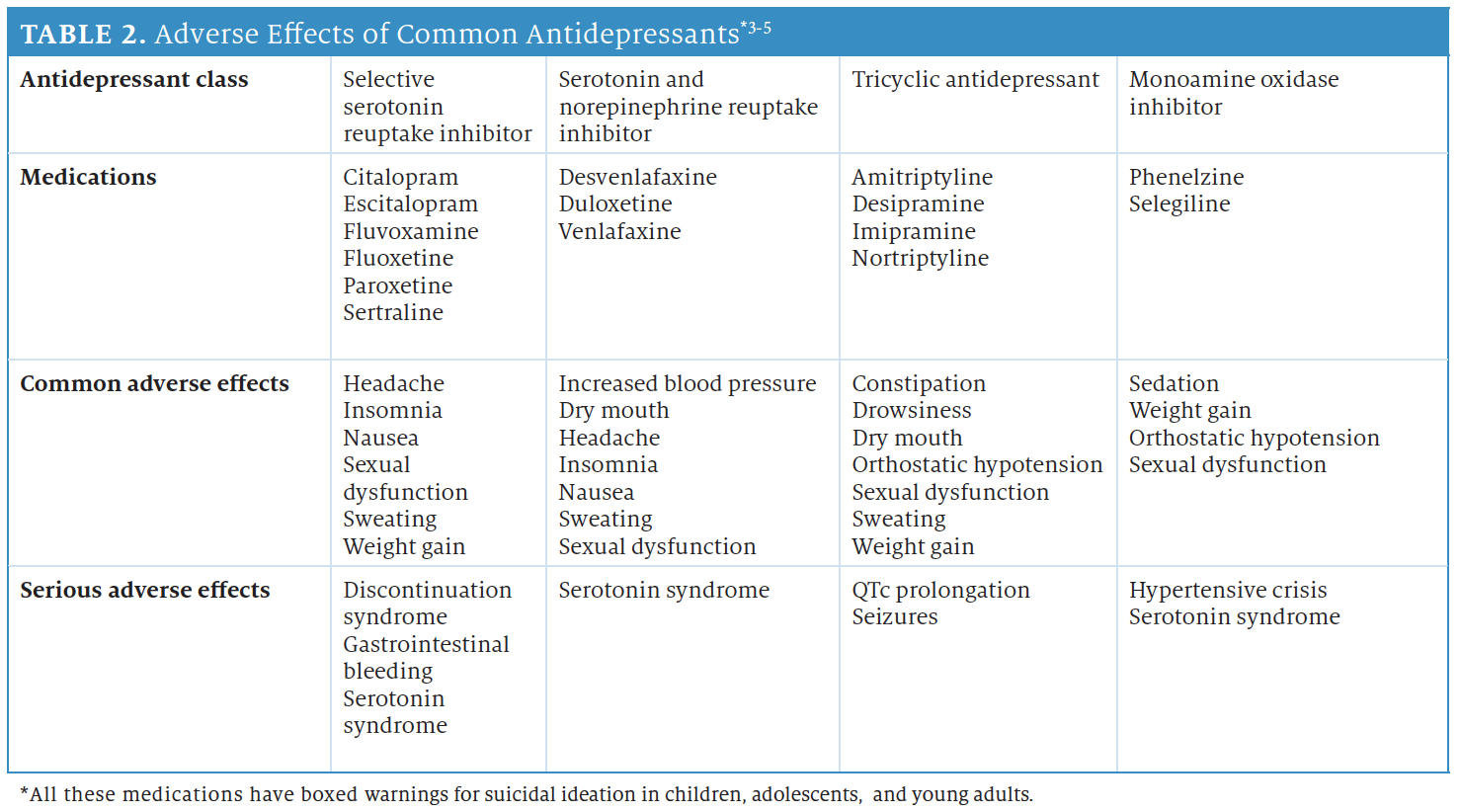
Medications used to treat depression include bupropion, a norepinephrine and dopamine reuptake inhibitor, and mirtazapine, an α2 blocker.5 Counsel patients that they may not notice positive changes from the antidepressant for 2 to 4 weeks.2 Also, monitor patients closely during the first 6 to 8 weeks, and increase the dose or switch therapies in patients who do not improve.3
DRUG-SPECIFIC CLINICAL PEARLS
Although many antidepressants have similar effects, a few have some
unique properties or adverse effects. These include the following:
- Paroxetine has anticholinergic properties, so avoid prescribing to elderly patients.6
- Fluoxetine and sertraline have active metabolites that can cause hepatic impairment. Both may cause restlessness or tremors.7,8
- Citalopram can cause QTc prolongation, requiring caution in patients with electrolyte imbalances.9
- Bupropion increases seizure risk.10
- Mirtazapine can increase appetite and weight gain.11
- Monoamine oxidase inhibitors should not be taken with fermented or preserved foods, as they may cause hypertensive crisis.3
TAPERING STRATEGIES
First-line therapy with antidepressants does not work for some patients. If it is necessary to switch therapy, tapering prevents serotonin syndrome and withdrawal symptoms. Cross-tapering gradually decreases the dose of the first antidepressant as the new antidepressant is initiated and titrated up over 1 to 2 weeks. A direct switch is when the prescriber stops an antidepressant and starts a new one This is usually possible between drugs of the same class.12
CONCLUSION
Pharmacists should mention additional ways patients can reduce the symptoms of depression. Remind patients to be active and exercise, avoid alcohol and nonprescription drugs, set realistic goals for themselves, and spend time with family and friends.13 Finally, pharmacists should advise patients to take their antidepressants at the same time every day for maximum benefit.3
ADDITIONAL PATIENT RESOURCES14
- Crisis Text Line: Text HOME to 741741
- MentalHealth.gov at www.mentalhealth.gov
- National Institute of Mental Health at www.nimh.nih.gov
- National Suicide Prevention Lifeline: Call 1-800-273-TALK (8255)
RAQUEL S. MATEUS is a PharmD candidate at the University of Connecticut School of Pharmacy in Storrs.
REFERENCES
- MalhiGS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2015;49(12):1087-1206. doi:10.1177/0004867415617657
- National Institute of Mental Health. Depression. National Institutes of Health. Updated February 2018. Accessed January 6, 2021. https://www.nimh.nih.gov/health/topics/depression/index.shtml
- American Psychological Association. APA guideline for the treatment of depression. February 16, 2019. Accessed January 13, 2021. https://www.apa.org/depression-guideline/guideline.pdf
- American Psychiatry Association. Treating major depressive disorder. October 2010. Accessed January 13, 2021. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd-guide.pdf
- Choudhry N, Fischer MA, Hoge E, et al. The pursuit of happiness: management of depression in the elderly a review for the practicing physician. Semantic Scholar. 2008. Accessed January 27, 2021. https://www.semanticscholar.org/paper/The-Pursuit-of-Happiness%3A-Management-of-Depression-Choudhry-Fischer/8a7212d4a3f3051fb4fb1425317c7436a3c8802c
- Paxil. Prescribing information. GlaxoSmithKline; 2011. Accessed January 13, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020031s067,020710s031.pdf
- Zoloft. Prescribing information. Pfizer; 2016.Accessed January 13, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/019839S74S86S87_20990S35S44S45lbl.pdf
- Prozac. Prescribing information. Eli Lilly and Company; 2017. Accessed January 13, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/018936s108lbl.pdf
- Celexa. Prescribing information. Forest Pharmaceuticals, Inc; 2011.Accessed January 13, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020822s042,021046s019lbl.pdf
- Wellbutrin.Prescribing information. GlaxoSmithKline; 2017. Accessed January 13, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/018644s052lbl.pdf
- Remeron.Prescribing information. Schering Corporation; 2007. Accessed January 27, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020415s023s024.pdf
- Keks N, Hope J, Keogh S. Switching and stopping antidepressants. AustPrescr. 2016;39(3):76-83. doi:10.18773/austprescr.2016.039
- American Psychiatric Association What is depression? October 2020. Accessed January 5, 2021. https://www.psychiatry.org/patients-families/depression/what-is-depression
- National Network of Depression Centers. Resource links. Accessed January 7, 2021.https://nndc.org/resource-links/