Depressive symptoms, mental wellbeing, and substance use among adolescents before and during the COVID-19 pandemic in Iceland: a longitudinal, population-based study
Adolescence represents a crucial developmental period in shaping mental health trajectories. In this study, we investigated the effect of the COVID-19 pandemic on mental health and substance use during this sensitive developmental stage.
Methods
In this longitudinal, population-based study, surveys were administered to a nationwide sample of 13–18-year-olds in Iceland in October or February in 2016 and 2018, and in October, 2020 (during the COVID-19 pandemic). The surveys assessed depressive symptoms with the Symptom Checklist-90, mental wellbeing with the Short Warwick Edinburgh Mental Wellbeing Scale, and the frequency of cigarette smoking, e-cigarette use, and alcohol intoxication. Demographic data were collected, which included language spoken at home although not ethnicity data. We used mixed effects models to study the effect of gender, age, and survey year on trends in mental health outcomes.
Findings
59 701 survey responses were included; response rates ranged from 63% to 86%. An increase in depressive symptoms (β 0·57, 95% CI 0·53 to 0·60) and worsened mental wellbeing (β −0·46, 95% CI −0·49 to −0·42) were observed across all age groups during the pandemic compared with same-aged peers before COVID-19. These outcomes were significantly worse in adolescent girls compared with boys (β 4·16, 95% CI 4·05 to 4·28, and β −1·13, 95% CI −1·23 to −1·03, respectively). Cigarette smoking (OR 2·61, 95% CI 2·59 to 2·66), e-cigarette use (OR 2·61, 95% CI 2·59 to 2·64), and alcohol intoxication (OR 2·59, 95% CI 2·56 to 2·64) declined among 15–18-year-olds during COVID-19, with no similar gender differences.
Interpretation
Our results suggest that COVID-19 has significantly impaired adolescent mental health. However, the decrease observed in substance use during the pandemic might be an unintended benefit of isolation, and might serve as a protective factor against future substance use disorders and dependence. Population-level prevention efforts, especially for girls, are warranted.
Funding
Icelandic Research Fund.
Translation
For the Icelandic translation of the abstract see Supplementary Materials section.
Introduction
The COVID-19 pandemic and the restrictions implemented to prevent and contain its transmission have caused widespread disruptions in the lives of adolescents and their families.
The psychological impact of quarantine and how to reduce it: rapid review of the evidence.
Initial findings on adolescent mental health during COVID-19 indicate cause for concern, with study findings suggesting an increase in depressive symptoms
What does adolescent substance use look like during the COVID-19 pandemic? Examining changes in frequency, social contexts, and pandemic-related predictors.
However, the rapidly accumulating evidence on the effect of COVID-19 on adolescent mental health has been limited by use of convenience samples and inadequate baseline measures to accurately capture the pandemic’s unfolding impact.
Says who? The significance of sampling in mental health surveys during COVID-19.
Research aimed at understanding how adolescent mental health is affected by COVID-19 is complex for several reasons. First, many psychiatric symptoms begin to emerge during adolescence. Any effects observed within the same study sample tracked over time could be confounded by the expected increase in mental health problems during this period. Second, the prevalence of mental health problems
Youth and young adult use of pod-based electronic cigarettes from 2015 to 2019: a systematic review.
have been increasing over the past 20 years; thus, prevalence measures from several pre-pandemic timepoints are necessary to disentangle the effect of COVID-19 from other recent trends in adolescent mental health. Third, adolescence is a developmental period marked by rapid biological and social changes, resulting in great age-dependent and gender-dependent variation. Accordingly, nuanced examination of this developmental period by chronological age and gender is necessary to inform targeted preventive intervention efforts. To overcome these challenges, studies with large and nationally representative samples are needed to compare same-age peers before and during the pandemic.
The Youth in Iceland study consists of extensive social surveys administered biennially nationwide to all 13–18-year-olds in Iceland who attend school.
Trends in depressive symptoms, anxiety symptoms and visits to healthcare specialists: a national study among Icelandic adolescents.
has shown that the self-rated depressive symptoms, mental wellbeing, and substance use measures assessed correspond to the prevalence of visits to paediatric psychiatrists and clinical child psychologists. We used data collected from 2016 to 2020 to assess whether changes in these outcomes during the pandemic exceeded expected changes from previous years (ie, from 2016 to 2018). The latest survey administration occurred Nov 20, 2020. During this time, Iceland was experiencing its third, and largest to date, wave of COVID-19 infections. The country was under strict physical-distancing mandates, with fewer than ten people allowed to gather simultaneously. Of particular relevance to adolescents, most secondary schools (students aged 16–18 years) were limited to online teaching, whereas earlier academic levels (≤16 years) continued to receive on-site learning in school. We aimed to examine the pandemic’s differential effects on adolescent mental health problems and substance use by chronological age and gender before and during the COVID-19 pandemic.
Research in context
Evidence before this study
We searched PubMed and Google Scholar for peer-reviewed papers published from Jan 1, 2020, to March 19, 2021, with the language restricted to English. In these databases, we paired the terms “COVID-19” and “coronavirus” with “mental health”, “psych*”, “depress*”, “well-being”, “substance use”, “alcohol”, and “nicotine”. The searches were then restricted to the following population: “adolescen*”, “child*”, and “youth”. We also followed up relevant references on child and adolescent mental health outcomes and substance use during COVID-19. Collectively, the existing studies suggested an increase in mental health problems, a decrease in e-cigarette use during the pandemic, and mixed findings on alcohol consumption. No previous studies tracked population-based prevalence of mental health outcomes and substance use over several years in order to disentangle potential effects of COVID-19 from recent upward trends in adolescent mental health problems and nicotine use. Furthermore, none analysed how adolescent outcomes during the pandemic differed by age and gender.
Added value of this study
This population-based study is, to our knowledge, the first to discern age-specific and gender-specific changes in the prevalence of adolescent mental health problems and substance use during the COVID-19 pandemic while accounting for previous upward trends in these outcomes. An increase in depressive symptoms and decrease in mental wellbeing scores and substance use were observed during the pandemic compared with same-age peers before the pandemic. Additionally, how adolescents fared during the pandemic differed by age and gender, with negative mental health outcomes being disproportionally reported by older adolescents (16–18-year-olds) and girls. We found a decline in rates of cigarette smoking, e-cigarette use, and alcohol intoxication among 15–18-year-old adolescents during the pandemic.
Implications of all the available evidence
Evidence in support of an increase in mental health problems among adolescents during COVID-19 is accumulating, with girls and older adolescents disproportionately negatively affected. Targeted interventions are needed to mitigate the negative impact of the pandemic on adolescent mental health.
Methods
Study design and participants
In this longitudinal, population-based study, we used data from the Youth in Iceland school surveys done by the Icelandic Centre for Social Research and Analysis (ICSRA)
Data collection procedures for school-based surveys among adolescents: The Youth in Europe Study.
in 2016, 2018, and 2020. Surveys were administered to 13–15-year-olds Feb 2–4, 2016 (n=11 774), Feb 6–8, 2018 (n=11 411), and Sept 14–Nov 20, 2020 (n=9836), and to 16–18-year-olds Oct 17–31, 2016 (n=9630), Oct 15–31, 2018 (n=9411), and Oct 6–Nov 20, 2020 (n=7639). The administration period was longer in 2020 to include all schools as some had to quarantine during the timeframe. Response rates of eligible participants ranged from 63–86%; full response data are available from the Icelandic Statistics Bureau. This study was approved by the National Bioethics Committee of Iceland (#21–038) and the Icelandic Data Protection Agency.
Procedures
All 13–15-year-olds and all 16–18-year-olds enrolled in post-secondary school in Iceland were invited to participate in the study. Consent forms were sent home to caregivers, who were asked to opt out of the study if they were not interested in their child participating. The survey was in Icelandic. During all administrations, students were asked to answer the survey anonymously. In 2016 and 2018, teachers distributed the paper-based questionnaires to all students present in class on the day of the survey, and who had not opted out of participating. Students returned the questionnaires sealed in blank envelopes. In 2020, teachers distributed a link to complete the electronic survey to all students present in class or in online class. Further methodological details are provided elsewhere.
(SCL-90) was used to measure depressive symptoms. Participants rated ten items on depressed mood in the previous week on a four-point Likert scale (from 1 [almost never] to 4 [often]). A composite score of these items was created, with higher scores suggesting higher levels of depressive symptoms (range 10–40). To gauge changes in the severity of depressive symptoms over time, cutoff scores based on the top 5% at the first timepoint (ie, 2016) by age and gender were created and classified as high depressive symptoms.
Measuring mental well-being in Denmark: validation of the original and short version of the Warwick-Edinburgh mental well-being scale (WEMWBS and SWEMWBS) and cross-cultural comparison across four European settings.
was used to measure mental wellbeing. Participants rated seven statements pertaining to self-worth, view towards the future, and social connectedness in the past 2 weeks on a five-point Likert scale (from 1 [none of the time] to 5 [all of the time]). A composite score was created for which higher scores indicated better mental wellbeing (range 7–35).
Participants rated the frequency of cigarette smoking (“How often have you smoked cigarettes in the past 30 days?”) and e-cigarette use (“How often have you used e-cigarettes in the past 30 days?”) during the past 30 days on a 7-point Likert scale (from 1 [never] to 7 [more than 40 times a day]). Participants rated the frequency of alcohol intoxication within the past 30 days on a six-point Likert scale (“How often have you been drunk in the past 30 days?”; from 1 [never] to 6 [more than 20 times]). The distribution of response rates according to these outcomes is provided in appendix 2 (pp 9–14). Each variable was dichotomised (never vs once or more).
Gender (boy vs girl vs other), household status (living with two parents or caregivers, vs other), and language spoken at home (only Icelandic spoken at home, vs other language spoken alone or with Icelandic) were used to assess the effect of gender, socioeconomic, and immigration differences on the outcomes. Ethnicity data were not collected. Health-care districts (coded from 1–7) were included as a random effect in all analyses to account for students nested within schools across the country.
Statistical analysis
Linear mixed effects models were generated for continuous outcomes (depressive symptoms and mental wellbeing) and logistic mixed effects models for binary outcomes (cigarette smoking, e-cigarette use, and alcohol intoxication). In all the models, chronological age and time (2016, 2018, and 2020) were grand-mean centred. Household status and language spoken within the home were added among the fixed effects as covariates. Health-care district was added as a random intercept to account for nesting of students within the schools. We used models with differing fixed effects to address each research aim.
In the first model, we examined whether increases in the outcomes during COVID-19 exceeded documented upward trends in these mental health problems and substance use among adolescents. This was done by entering time as a fixed effect in predicting each outcome.
Second, we investigated the differential effect of COVID-19 by chronological age. We entered the main and interactive effects of time and age as fixed effects for each outcome. We explored differences in outcomes in 2016 and 2018 for each age group and then compared these rates to those in 2020.
Third, gender differences were examined with a model in which the main effect and interaction between gender and time were entered as fixed effects. Following these analyses, the interactive effect of time and age on each outcome was examined separately for adolescent girls and boys.
To gauge the strength of the findings, standardised mean differences were created for each outcome by time using an effect size calculator and reported as Cohen’s d. For continuous outcomes, the means and SDs from 2020 were compared with these values in 2016 and 2018. To calculate Cohen’s d for binary outcomes, two-by-two frequency tables were created in which the event proportions (eg, endorsement of substance use) in 2020 were compared with the combined event proportions in 2016 and 2018. A positive value indicated an increase in the means or prevalence in 2020 compared with pre-COVID-19, while a negative value indicated a decrease. Lastly, correlations were conducted to examine differences in the relationship between mental health outcomes and the substance abuse outcomes by time (appendix 2 p 15).
Applying Bonferroni corrections for multiple testing, the models were considered significant at a p value of less than 0·003. The mixed effect models were conducted using the lme4 package
All data analyses and visualisations were done with R version 3.6.0.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
Table 1 shows the sample sizes and demographic characteristics for all study participants at the time of survey administration. Consistent with increases in immigration to Iceland, the percentage of youth for whom Icelandic was not the primary language spoken at home increased across time (p
Table 1Demographic characteristics
Data are n (%). All participants in 2016 and 13–15 year-olds in 2018 were provided with only the male or female response options when reporting gender. Geographical location of residence was obtained from the Icelandic health-care district codes (1=within the capital area, >1=outside the capital area).
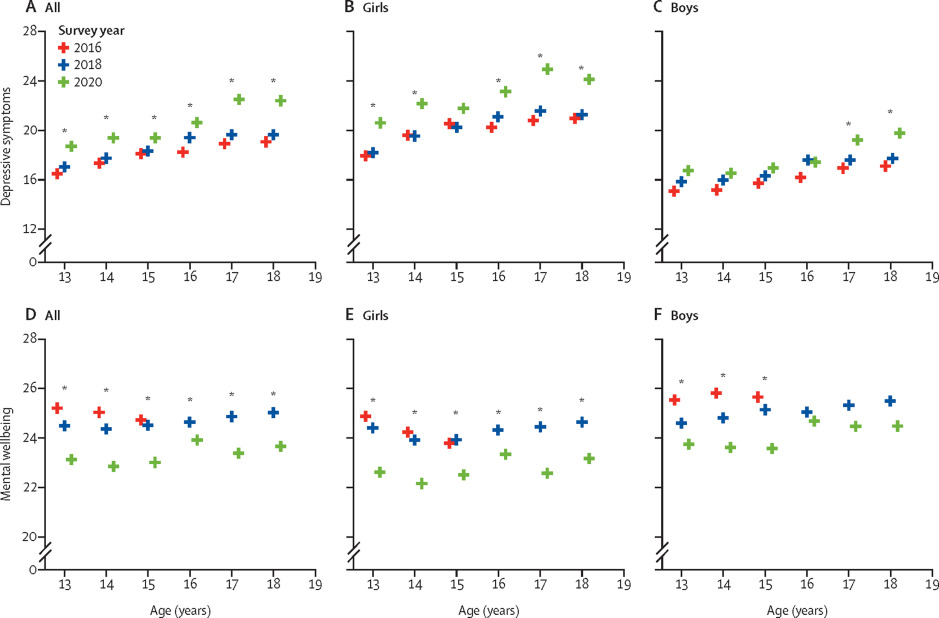
Significantly higher depressive symptoms were reported by participants in 2020 than in 2016 and 2018 for all age groups (ptable 2). Adjusting for gender and household status, depressive symptoms among 13–18-year-olds significantly increased over time, from a mean of 17·96 (SD 7·53) in 2016 to 18·54 (7·52) in 2018 and 20·30 (7·98) in 2020, an increase of 3·2% between 2016 and 2018 and of 9·5% between 2018 and 2020 (β 0·57, 95% CI 0·53–0·60). Age and the interaction between age and time also significantly predicted depressive symptoms (figure 1, table 3). No significant differences in depressive symptoms between 2016 and 2018 across age groups were found (p>0·030; appendix 2 pp 4–7), with the exception of 16-year-olds, in whom higher depressive symptoms were reported in 2018 than in 2016 (p
Table 2Depressive symptoms, mental wellbeing, and substance use for each age group by time of the survey administration
Data are N, mean (SD), or n (%), unless otherwise specified.
Youth not identifying as boy or girl were not included in the stratified analyses because the response option of “other” was not available in the survey for 13–15-year-olds in 2016 and 2018 or for 16–18-year-olds in 2016. *Significant difference for 2020 vs previous years at pappendix 2 (pp 4–7).
Table 3Effects of time, age, and their interaction on study outcomes
The analyses are linear and logistic mixed effects models adjusted for household status, primary language spoken at home, and residency.
Higher depressive symptoms were observed in girls in 2020 compared with 2016 and 2018 across age groups (p=0·0018; appendix 2 pp 4–7). The interaction between gender and time significantly predicted depressive symptoms (β 0·027, 95% CI 0·20–0·35). In the stratified analyses, age, time, and the interaction between age and time significantly predicted depressive symptoms in girls (figure 1, table 3). Similar depressive symptoms were reported among girls in 2016 and 2018 across the age groups (p=0·35; appendix 2 pp 4–7). For boys, age and time significantly predicted depressive symptoms, but the interaction between age and time did not (figure 1, table 3).
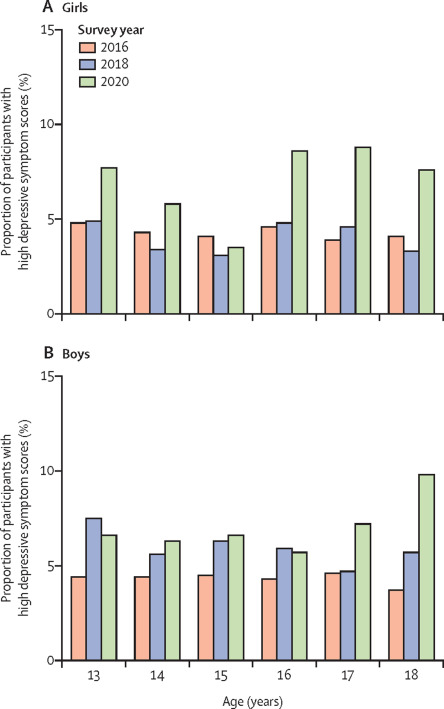
We next examined change in the proportion of individuals with high depressive symptom scores, defined as greater than or equal to the 5th centile in the 2016 cohort for each age group. A significantly higher proportion of girls across all age groups reported high depressive symptom scores during the pandemic compared with previous timepoints (2016 and 2018; pfigure 2). However, this effect was only observed among 17-year-old and 18-year-old boys (pfigure 2).
Figure 2Proportion of participants with high depressive symptom scores
Figure shows the proportion of individuals with depressive symptom scores equal to or above those of the 5th centile determined separately for boys and girls for each age group in 2016.
Mental wellbeing significantly worsened over time among 13–18-year-olds (β −0·46, 95% CI −0·49 to −0·42), with an average decrease of 1·6% between 2016 and 2018 (mean score 25·04 [SD 5·94] in 2016 vs 24·62 [5·64] in 2018), compared with 5·4% between 2018 and 2020 (mean score 23·29 [5·43] in 2020). Age and time significantly predicted mental wellbeing; however, the interaction between age and time was not significantly associated with mental wellbeing (figure 1, table 3), with significantly worsened mental wellbeing across all age groups during the pandemic compared with same-age peers in 2016 and 2018 (Cohen’s d ranging from −0·35 to −0·20; table 2, figure 1).
For the gender analyses, time (β −0·045, 95% CI −0·49 to −0·40) and gender (β −1·13, 95% CI −1·23 to −1·03) were significant predictors of mental wellbeing, with mental wellbeing worsening over time and girls reporting overall lower mental wellbeing than boys. The interaction between gender and time did not predict mental wellbeing (β 0·020, 95% CI −0·05 to 0·08), indicating that mental wellbeing was similarly affected in adolescent girls and boys during COVID-19. In the gender-stratified analyses, significantly worse mental wellbeing was observed across age groups in 2020 compared with 2016 and 2018 for both girls and boys (ptable 3, figure 1).
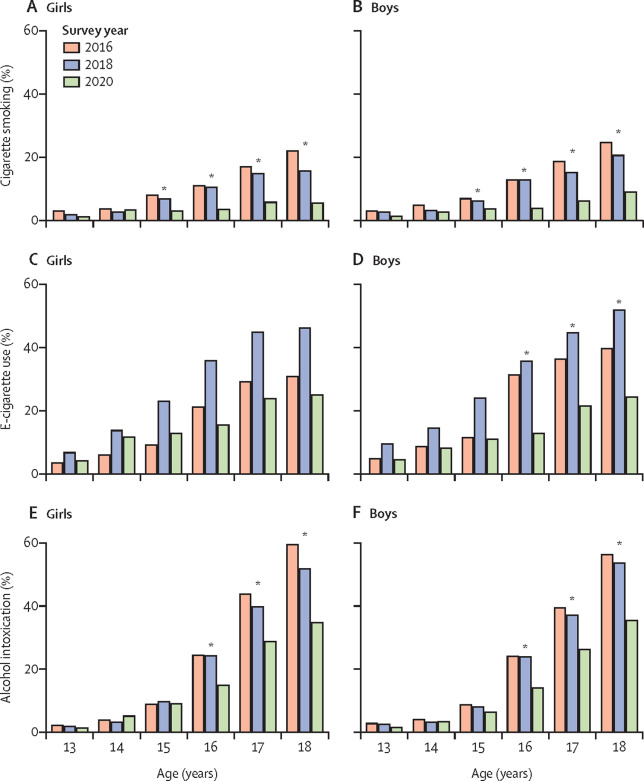
Similar rates of cigarette smoking were reported among 13–17-year-olds in 2016 to 2018 (p>0·16; appendix 2 pp 4–7), while a significant decrease in cigarette smoking was observed among 18-year-olds in 2018 compared with 2016. When examining cigarette smoking in 2020, no differences were noted among 13-year-olds and 14-year-olds compared with 2016 and 2018. However, a significant decrease in cigarette smoking was observed among 15–18-year-olds in 2020 compared with 2016 and 2018 (Cohen’s d ranging from −0·72 to −0·08; table 2). Overall, substantially fewer adolescents reported cigarette smoking in the past 30 days in 2020 (664 [3·8%] of 17 475) compared with 2018 (1832 [8·8%] of 20 822) and 2016 (2226 [10·4%] of 21 404; OR 0·79, 95% CI 0·77–0·80). Age, time, and the interaction between age and time significantly predicted cigarette smoking (table 3).
We found that gender (OR 0·88, 95% CI 0·83–0·94) and time (OR 0·79, 95% CI 0·77–0·81) significantly predicted cigarette smoking, but the interaction between time and gender did not (OR 0·98, 95% CI 0·95–1·02). The finding suggests similar decreases in cigarette smoking among adolescent boys and girls across time (table 3). The gender-stratified analyses demonstrated significant main and interaction effects for age and time in predicting cigarette smoking for adolescent girls. For boys, the main effect of age and time significantly predicted cigarette smoking, but not their interaction. Similar decreases in cigarette smoking were reported among 15–18-year-old girls and boys in 2020 compared with 2016 and 2018, with greater decreases in cigarette smoking corresponding to higher chronological age (figure 3A–B).
Figure 3Frequency of cigarette smoking, e-cigarette use, and alcohol intoxication in the past 30 days
Youth not identifying as boy or girl were not included in the stratified analyses because the response option of “other” was not available in the survey for 13–15-year-olds in 2016 and 2018 or for 16–18-year-olds in 2016. *Significant difference for 2020 vs previous years at pappendix 2 (pp 4–7).
E-cigarette use was higher in 2018 compared with 2016 across all age groups (ptable 2). Significant differences over time were observed in the proportion of 13–18-year-olds who reported e-cigarette use within the past 30 days (OR 0·95, 95% CI 0·94–0·96). Specifically, 3789 (17·7%) of 21 404 adolescents reported e-cigarette use in 2016 compared with 5705 (27·4%) of 20 822 in 2018 and 2360 (13·5%) of 17 475 in 2020. Age, time, and the interaction between age and time significantly predicted e-cigarette use in 13–18-year-old adolescents (table 3).
The gender analyses showed that time (OR 0·90, 95% CI 0·88–0·91) and the interaction between gender and time significantly predicted e-cigarette use (OR 1·11, 95% CI 1·09–1·14), whereas the main effect of gender (OR 0·94, 95% CI 0·90–0·98) did not. The findings suggested greater decreases in e-cigarette use among 13–18 year-old boys than girls over time. The gender stratified analyses revealed significant main effects of age and interaction effects of time and age for girls and boys (table 3, figure 3C–D). Significant decreases in e-cigarette use among 15–18-year-olds in 2020 compared with 2016 and 2018 were noted for both genders, although this decrease was greater among boys compared with girls.
Alcohol intoxication among 13–18-year-olds significantly differed by time (OR 0·88, 95% CI 0·87–0·90), with similar rates in 2016 and 2018 (4409 [20·6%] of 21 404 in 2016; and 4060 [19·5%] of 20 822 in 2018) but significantly lower rates in 2020 (2307 [13·2%] of 17 475).
Age, time, and the interaction between age and time significantly predicted alcohol intoxication (table 3). Similar levels of alcohol intoxication were reported across age groups in 2016 and 2018 (p>0·0079; appendix 2 pp 4–7). Decreases in alcohol intoxication were observed among 15–18-year-olds during 2020 compared with 2016 and 2018 (ptable 2).
In the gender × time interaction model, gender (OR 1·12, 95% CI 1·07–1·17) and time (OR 0·87, 95% CI 0·86–0·89) were significant, with higher levels of alcohol intoxication reported by adolescent girls. Similar patterns were observed in the gender-stratified analyses (table 3). A decrease in alcohol intoxication occurred among 16–18-year-old girls and boys (pfigure 3E–F).
Discussion
Our findings show that depressive symptoms and the mental wellbeing of adolescents in Iceland have worsened during the COVID-19 pandemic, beyond the increase expected on the basis of previous trends, although substance use has decreased. Adolescents aged 16–18 years are the most negatively affected. This might be explained, partly, by the differences in the social restrictions implemented in compulsory and post-secondary schools at the time of data collection. Specifically, 16–18-year-olds in Iceland experienced high levels of disruption in instructional mode and school schedules, with most classes switching to online instruction, whereas 13–15-year-olds mostly continued to participate in on-site instruction at school. Outside of school, similar social restrictions applied to all age groups. During this time, the country was under strict physical distancing mandates, with fewer than ten people allowed to gather at once, organised sports and group activities suspended, and restaurants and bars closed. However, the need for autonomy and peer interactions is generally greater for 16–18-year-olds than for 13–15-year-olds.
We found greater increases in depressive symptoms and decreases in mental wellbeing among adolescent girls compared with boys. Multiple biological and social factors could account for these findings. For example, hormonal influences during puberty increase sensitivity to interpersonal stressors among adolescent girls,
Sexual selection and sex differences in the prevalence of childhood externalizing and adolescent internalizing disorders.
and adolescent girls are more likely than their male counterparts to engage in social behaviours that exacerbate depressive symptoms in response to stress, such as the tendency to extensively discuss problems in dyadic relationships.
Why is depression more common among women than among men?.
This study revealed a decline in cigarette smoking, e-cigarette use, and alcohol intoxication among 15–18-year-old adolescents during the COVID-19 pandemic. Consistent with social developmental theories on adolescent substance use, the social restrictions implemented to prevent the spread of COVID-19 might have resulted in less social pressure and fewer rewards of exploring substance use.
Different factors predict adolescent substance use versus adult substance abuse: lessons from a social-developmental approach.
Additionally, a public health campaign warning adolescents of the health risks of e-cigarette use has been conducted within the national school system. In parallel with these efforts, considerable media coverage has highlighted the general health risks associated with e-cigarette use and increased COVID-19 symptoms and complications among infected habitual users compared with non-users. Thus, for e-cigarette use it is impossible to disentangle the effect of the campaign and media coverage from the effect of the pandemic. Notwithstanding, the observed decrease in e-cigarette use may confer some protection against future substance use disorders and dependence, which frequently emerge during adolescence.
Research review: what have we learned about adolescent substance use?.
Further research is needed to determine the long-term effect.
This study has strengths in terms of its sample size, population reach, and design, but also some limitations. We used self-reported depressive symptoms: research is needed to determine whether clinically relevant levels of depression have increased and to establish the long-term effect of the pandemic on mental health outcomes and substance use. Yet, our previous work has demonstrated that self-reported depressive symptoms correspond to the prevalence of visits to paediatric psychiatrists and clinical child psychologists.
Trends in depressive symptoms, anxiety symptoms and visits to healthcare specialists: a national study among Icelandic adolescents.
As such, although our findings cannot be interpreted as evidence of an increase in levels of clinical depression, they are concerning and probably reflect an actual increase in mental health problems.
The seasonal timing of the survey administration among 13–15-year-olds differed in 2020 from the administrations in 2016 and 2018. Given Iceland’s geographical location, higher levels of mental health problems during the winter months could be expected. However, 13–15-year-olds reported higher depressive symptoms during autumn administration (October, 2020) compared with winter administration (February, 2016 and 2018). Thus, it is possible that the increase in mental health problems among 13–15-year-olds during COVID-19 would have been greater if both measurements had occurred during the same time of year. Furthermore, in an effort to disentangle the effect of COVID-19 from the expected upward trend in mental health problems, we compared changes in mental health problems from 2016 to 2018 with those occurring between 2018 and 2020. Although our study design provides a clearer picture of the potential effects of the pandemic than previous studies, we cannot exclude the possibility that other societal factors, unrelated to COVID-19, could have contributed to the observed increase in mental health problems.
Moreover, the findings cannot be generalised to 16–18-year-old adolescents not enrolled in post-secondary schools (5–18% of the population), who are probably at greater risk for psychiatric disorders than those pursuing further education. Additionally, 5–19% of eligible individuals opted out of participating or were not present at the time of survey administration (appendix 2 p 8). Given that the school surveys were administered biennially at the population level, there is overlap between participants across years, which might affect the findings. However, due to the anonymity of the participants or no available information, we were unable explore these issues and statistically adjust for them.
Compared with many other countries, pandemic-related social restrictions in Iceland have been minimal. Increased social restrictions implemented elsewhere will probably produce even greater effects on mental health. Our findings represent a conservative estimate of impaired adolescent wellbeing during COVID-19. Additional studies, especially those using samples stratified by gender, are needed to determine how youth are differentially affected by the varying social restrictions and cultural factors that could affect coping mechanisms during times of uncertainty. Meanwhile, population-level prevention efforts, especially for girls, are warranted. Furthermore, the effect of the pandemic on mental health and substance use is likely to be more pronounced among other subgroups, such as youth living in poverty or with pre-existing mental health conditions. With research rapidly emerging on these important issues,
Interventions to ameliorate the psychosocial effects of the COVID-19 pandemic on children—a systematic review.
more targeted interventions can be developed to mitigate the negative impact of the pandemic on adolescent mental health.
TH and IET conceived the research question and design, ran all analyses, and wrote the first draft of the Article. IDS, JS, EMJT, and IET identified the measurements used the survey in 2018 and 2020 and coordinated its administration to all secondary and post-secondary schools in Iceland. BBA, ALK, HBV, JPA, and IDS reviewed drafts and edited the Article. All authors approved the final draft. All authors had full access to all data in the study and had final responsibility for the decision to submit for publication.