
The consequences of hearing loss are many, including social isolation1-3 and depression.10-13 The failure of hearing aids to either prevent or improve depression may stem from a complex relationship between hearing loss, depression, and the social dynamism of hearing loss that we have yet to fully understand. To this end, there are several opportunities to explore the relationship between hearing loss and depression. Moreover, there may be utility in identifying depression in patients with hearing loss at the point of care considering the established link between hearing loss and depression.

Shutterstock/Photographee.eu, technology. Hearing loss, mental health.
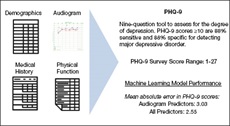
Using machine learning to predict depression scores (adapted from Crowson et. al., 2020). Technology. Hearing loss, mental health.
The primary objective of our work was to use a predictive approach using machine learning and audiometric data to determine if these data accurately predict patient-reported depression. We hypothesized that an advanced machine learning model may be useful for identifying depression in patients with audiometric data. We also sought to determine if the addition of other clinical and demographic variables combined with the audiometric data would produce further gains in model accuracy.
STUDY HIGHLIGHTS
In our study, we developed a supervised machine learning model using National Health and Nutrition Examination Survey (NHANES) data, composed of subjective and objective audiometric variables and several other health determinant predictors, to predict scores on a validated depression scale—the Patient Health Questionnaire (PHQ-9). The NHANES is a cross-sectional public health survey designed to assess the health and nutrition status of individuals in the United States. NHANES data has been used in numerous research investigations to incorporate the interplay between determinants of health and specific medical conditions.
In a sample of participants from a survey cycle of the NHANES database, our supervised machine learning approach accurately predicted depression scale scores using audiometric and health determinant predictors. The model’s most influential audiometric predictors of higher scores on the depression scale were functional dimensions and not objective audiometric testing variables. Among the most influential predictors, half were related to the social dynamics of hearing loss. The remaining predictors associated with depression in hearing loss were related to noise exposure, tinnitus, and objective audiometric testing. When expanding to include predictors ranging from demographics to other medical and health status content, a social context of hearing loss ranked in the top five most influential.
IMPLICATIONS
A strong association between social isolation and hearing loss has been demonstrated in adults.1-3 The observation that hearing loss leads to social isolation is intuitive given that hearing loss leads to impaired efficiency of communication. The connection between social isolation and depression is a natural extension as humans are social creatures.
If hearing care professionals treat hearing loss with conventional hearing aid devices, would it be reasonable to expect social isolation and associated depression to improve? Unfortunately, the relationship appears more complex. Prior work has shown that hearing aids do not result in consistent improvement in social isolation11,14 or depression.10-13 Perhaps the disconnect might be explained by noting that hearing amplification exclusively does not address hearing performance in real-life social situations. Basic sound amplification can and does help individuals with hearing loss. More advanced hearing aids incorporate signal processing technologies to better isolate the “relevant” sounds in noisy environments. Perhaps future research involving hearing aids with enhanced signal processing technology may lead to further insights into the utility of hearing aids to directly augment the social dynamics of hearing loss.
In summary, we found the NHANES dataset is useful for training machine learning models to accurately predict depression scale scores from audiometric data. As many of the variables collected in the NHANES data are the same clinical data we extract from our patients in real-life clinical encounters, such a predictive model could be useful in predicting depression scale scores at the point of care. We found the most influential audiometric predictors of higher scores on the depression scale were functional dimensions of hearing loss and not simply objective audiometric data like thresholds and word recognition scores. Among these influential functional dimensions, our model indicated the specific effect of hearing loss on social relations was particularly powerful. This is an interesting finding, as prior investigations into the effect of hearing aids on depression and social isolation have failed to show a consistent benefit. Simply giving a patient a hearing aid is not a guarantee that social isolation or depression will improve. Thus, our model output puts forth a new hypothesis that simply amplifying sound alone, in general, fails to address or improve the social dynamism of hearing loss. For today’s hearing care clinicians, we suggest that recognizing that social aspects of hearing loss may carry more influence on the development or maintenance of depression than previously thought. Moreover, we may need to reimagine our aural rehabilitation strategies to include specific interventions to optimize social dynamics.
REFERENCES